Overview
 An Achilles tendon rupture, or tear, is a common condition. This typically occurs in the unconditioned individual who sustains the rupture while playing sports, or perhaps, from tripping. There is a vigorous contraction of the muscle and the tendon tears.
An Achilles tendon rupture, or tear, is a common condition. This typically occurs in the unconditioned individual who sustains the rupture while playing sports, or perhaps, from tripping. There is a vigorous contraction of the muscle and the tendon tears.
Causes
Achilles tendon ruptures are most likely to occur in sports requiring sudden stretching, such as sprinting and racquet sports. Achilles tendon ruptures can happen to anyone, but are most likely to occur to middle age athletes who have not been training or who have been doing relatively little training. Common sporting activities related to Achilles tendon rupture include, badminton, tennis, squash. Less common sporting activities that can lead to Achilles tendon rupture include: TKD, soccer etc. Occasionally the sufferer may have a history of having had pain in the Achilles tendon in the past and was treated with steroid injection to around the tendon by a doctor. This can lead to weakening of the tendon predisposing it to complete rupture. Certain antibiotics taken by mouth or by intravenous route can weaken the Achilles tendon predisposing it to rupture. An example would be the quinolone group of antibiotics. An common example is Ciprofloxacin (or Ciprobay).
Symptoms
The most common initial symptom of Achilles tendon rupture is a sudden snap at the back of the heels with intense pain. Immediately after the rupture, the majority of individuals will have difficult walking. Some individuals may have had previous complains of calf or heel pain, suggesting prior tendon inflammation or irritation. Immediately after an Achilles tendon rupture, most individuals will develop a limp. In addition, when the ankle is moved, the patient will complain of pain. In all cases, the affected ankle will have no strength. Once the Achilles tendon is ruptured, the individual will not be able to run, climb up the stairs, or stand on his toes. The ruptured Achilles tendon prevents the power from the calf muscles to move the heel. Whenever the diagnosis is missed, the recovery is often prolonged. Bruising and swelling around the calf and ankle occur. Achilles tendon rupture is frequent in elderly individuals who have a sedentary lifestyle and suddenly become active. In these individuals, the tendon is not strong and the muscles are deconditioned, making recovery more difficult. Achilles tendon rupture has been reported after injection of corticosteroids around the heel bone or attachment of the tendon. The fluoroquinolone class of antibiotics (such as ciprofloxacin [Cipro]) is also known to cause Achilles tendon weakness and rupture, especially in young children. Some individuals have had a prior tendon rupture that was managed conservatively. In such cases, recurrence of rupture is very high.
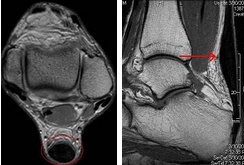
Diagnosis
Your doctor diagnoses the rupture based on symptoms, history of the injury and physical examination. Your doctor will gently squeeze the calf muscles, if the Achilles tendon is intact, there will be flexion movement of the foot, if it is ruptured, there will be no movement observed.
Non Surgical Treatment
Achilles tendon rupture is treated using non surgical method or surgical method. Non surgical treatment involves wearing a cast or special brace which is changed after some period of time to bring the tendon back to its normal length. Along with cast or brace, physical therapy may be recommended to improve the strength and flexibility of leg muscles and Achilles tendon.
Surgical Treatment
Most published reports on surgical treatment fall into 3 different surgical approach categories that include the following: direct open, minimally invasive, and percutaneous. In multiple studies surgical treatment has demonstrated a lower rate of re-rupture compared to nonoperative treatment, but surgical treatment is associated with a higher rate of wound healing problems, infection, postoperative pain, adhesions, and nerve damage. Most commonly the direct open approach involves a 10- to 18-cm posteromedial incision. The minimally invasive approach has a 3- to 10-cm incision, and the percutaneous approach involves repairing the tendon through multiple small incisions. As with nonsurgical treatment there exists wide variation in the reported literature regarding postoperative treatment protocols. Multiple comparative studies have been published comparing different surgical approaches, repair methods, or postoperative treatment protocols.
An Achilles tendon rupture, or tear, is a common condition. This typically occurs in the unconditioned individual who sustains the rupture while playing sports, or perhaps, from tripping. There is a vigorous contraction of the muscle and the tendon tears.Causes
Achilles tendon ruptures are most likely to occur in sports requiring sudden stretching, such as sprinting and racquet sports. Achilles tendon ruptures can happen to anyone, but are most likely to occur to middle age athletes who have not been training or who have been doing relatively little training. Common sporting activities related to Achilles tendon rupture include, badminton, tennis, squash. Less common sporting activities that can lead to Achilles tendon rupture include: TKD, soccer etc. Occasionally the sufferer may have a history of having had pain in the Achilles tendon in the past and was treated with steroid injection to around the tendon by a doctor. This can lead to weakening of the tendon predisposing it to complete rupture. Certain antibiotics taken by mouth or by intravenous route can weaken the Achilles tendon predisposing it to rupture. An example would be the quinolone group of antibiotics. An common example is Ciprofloxacin (or Ciprobay).
Symptoms
The most common initial symptom of Achilles tendon rupture is a sudden snap at the back of the heels with intense pain. Immediately after the rupture, the majority of individuals will have difficult walking. Some individuals may have had previous complains of calf or heel pain, suggesting prior tendon inflammation or irritation. Immediately after an Achilles tendon rupture, most individuals will develop a limp. In addition, when the ankle is moved, the patient will complain of pain. In all cases, the affected ankle will have no strength. Once the Achilles tendon is ruptured, the individual will not be able to run, climb up the stairs, or stand on his toes. The ruptured Achilles tendon prevents the power from the calf muscles to move the heel. Whenever the diagnosis is missed, the recovery is often prolonged. Bruising and swelling around the calf and ankle occur. Achilles tendon rupture is frequent in elderly individuals who have a sedentary lifestyle and suddenly become active. In these individuals, the tendon is not strong and the muscles are deconditioned, making recovery more difficult. Achilles tendon rupture has been reported after injection of corticosteroids around the heel bone or attachment of the tendon. The fluoroquinolone class of antibiotics (such as ciprofloxacin [Cipro]) is also known to cause Achilles tendon weakness and rupture, especially in young children. Some individuals have had a prior tendon rupture that was managed conservatively. In such cases, recurrence of rupture is very high.
Diagnosis
Your doctor diagnoses the rupture based on symptoms, history of the injury and physical examination. Your doctor will gently squeeze the calf muscles, if the Achilles tendon is intact, there will be flexion movement of the foot, if it is ruptured, there will be no movement observed.
Non Surgical Treatment
Achilles tendon rupture is treated using non surgical method or surgical method. Non surgical treatment involves wearing a cast or special brace which is changed after some period of time to bring the tendon back to its normal length. Along with cast or brace, physical therapy may be recommended to improve the strength and flexibility of leg muscles and Achilles tendon.
Surgical Treatment
Most published reports on surgical treatment fall into 3 different surgical approach categories that include the following: direct open, minimally invasive, and percutaneous. In multiple studies surgical treatment has demonstrated a lower rate of re-rupture compared to nonoperative treatment, but surgical treatment is associated with a higher rate of wound healing problems, infection, postoperative pain, adhesions, and nerve damage. Most commonly the direct open approach involves a 10- to 18-cm posteromedial incision. The minimally invasive approach has a 3- to 10-cm incision, and the percutaneous approach involves repairing the tendon through multiple small incisions. As with nonsurgical treatment there exists wide variation in the reported literature regarding postoperative treatment protocols. Multiple comparative studies have been published comparing different surgical approaches, repair methods, or postoperative treatment protocols.
